Case Author: Dmitry Nikolaev
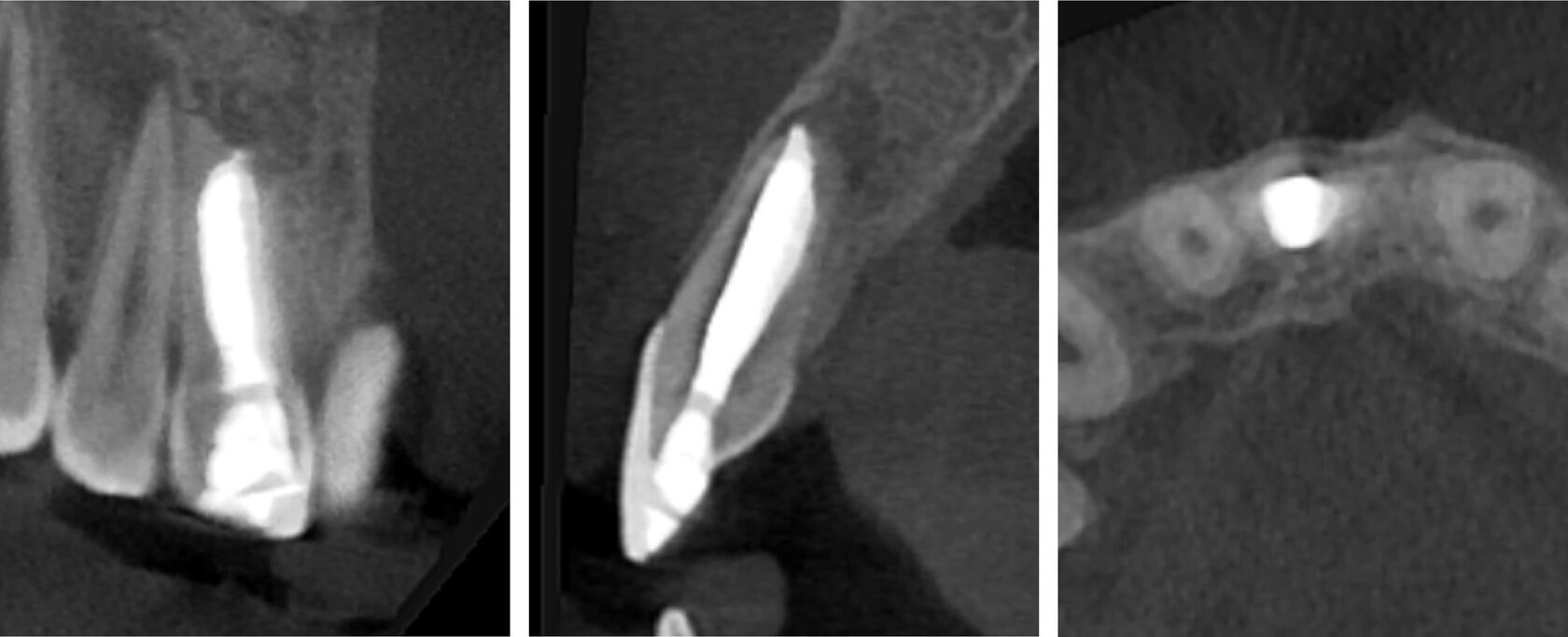
1. A pediatric patient presented with a history of dental trauma occurring approximately five years prior, for which no timely treatment had been provided. (Image 1)

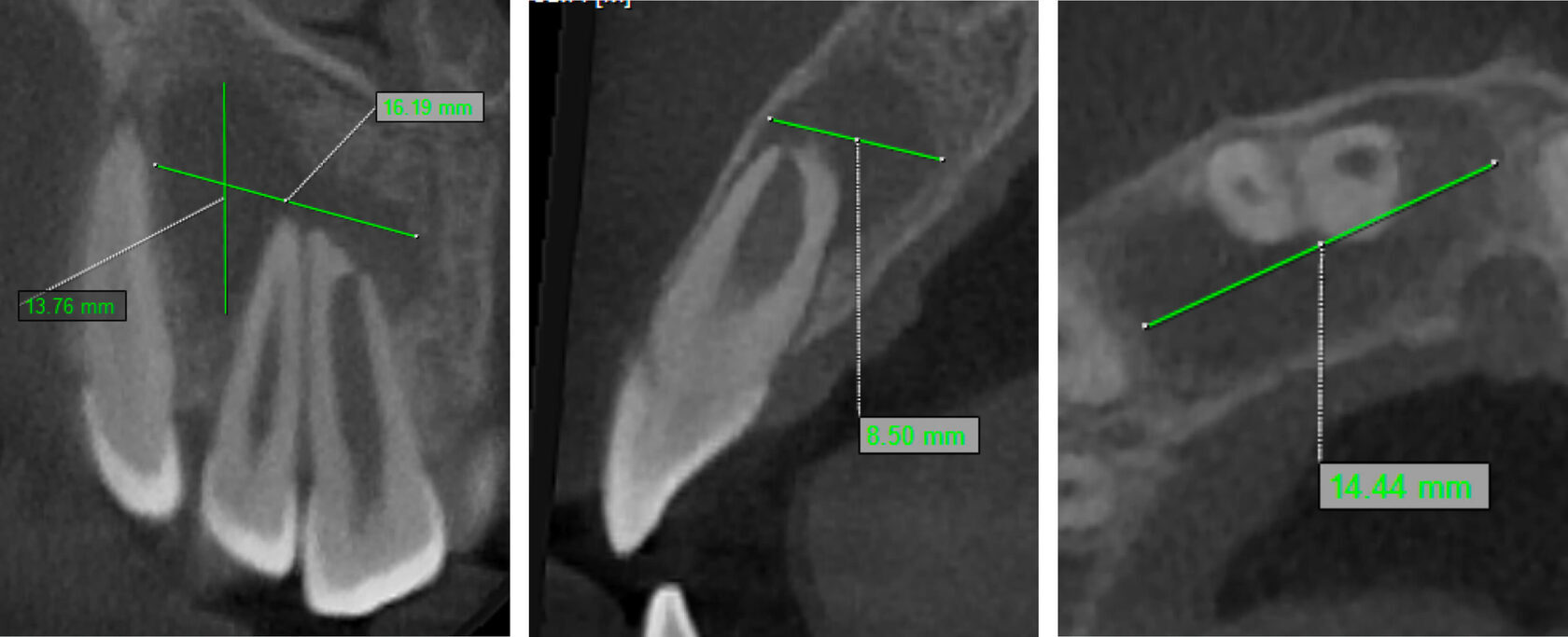
2. Tooth #11 was diagnosed as non-vital with apical periodontitis, presenting extensive periapical bone destruction radiographically. In contrast, tooth #12 responded normally to vitality tests, confirming pulp vitality. (Image 2,3,4)
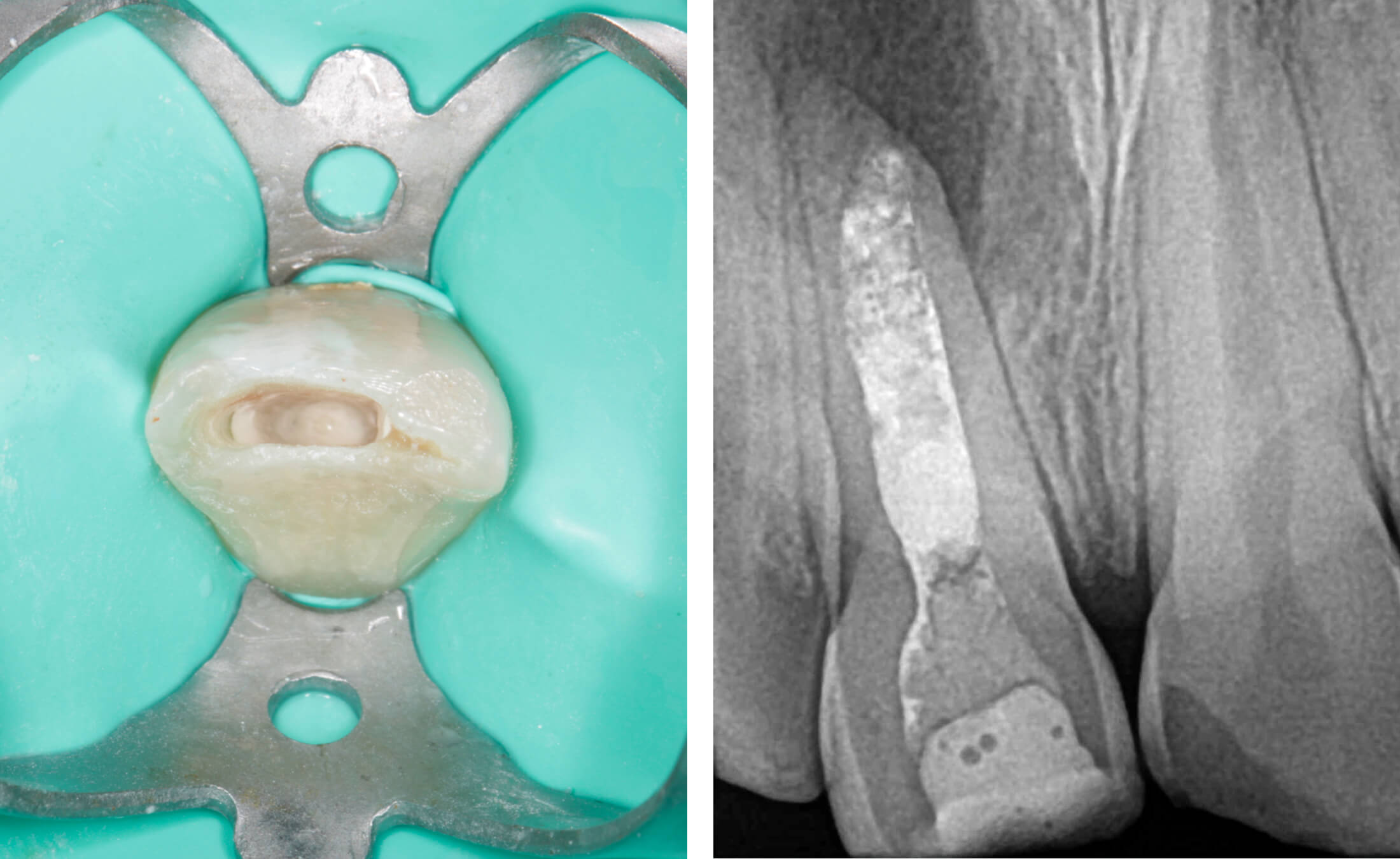
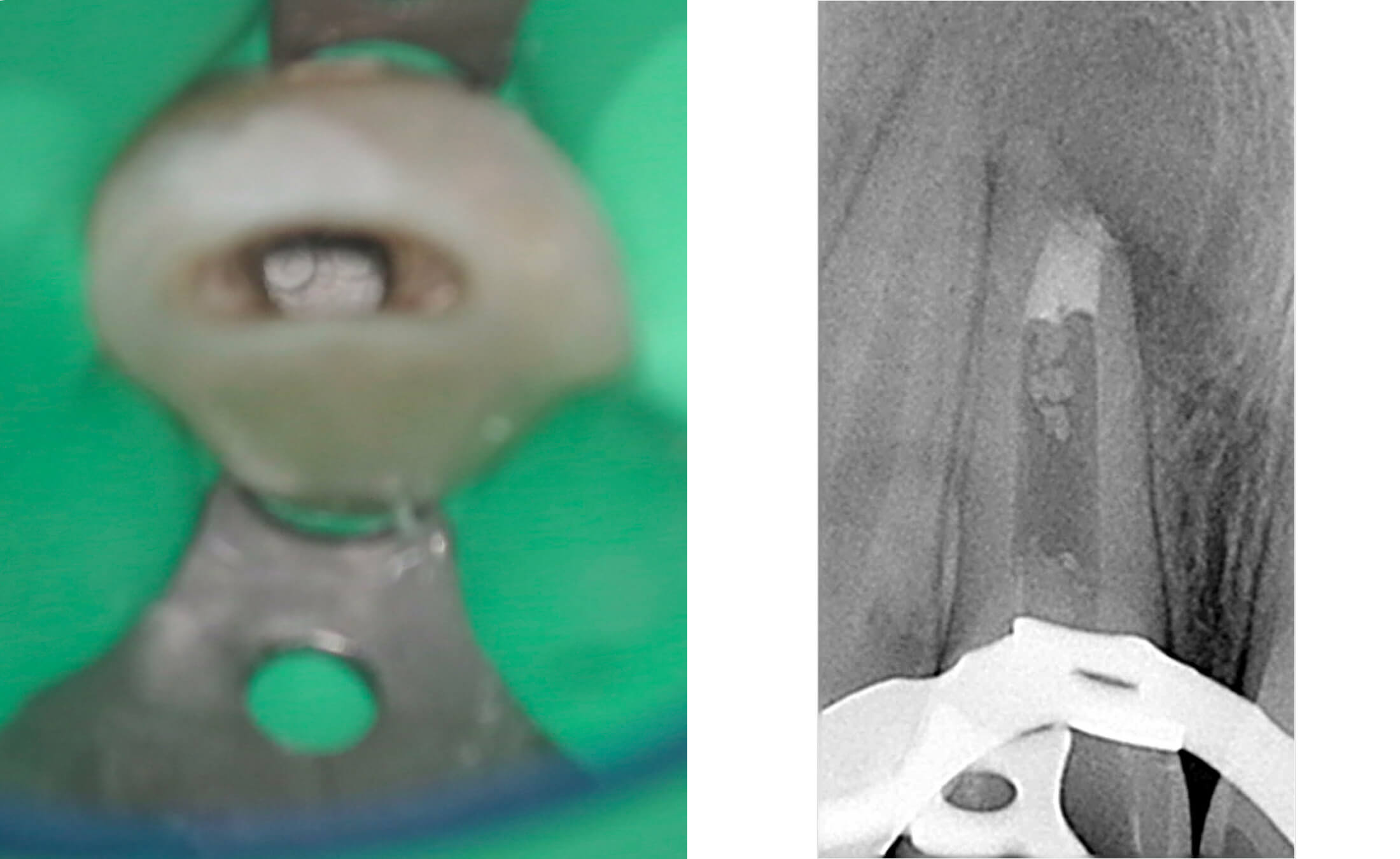
3. During the initial appointment, an endodontic access cavity was prepared, followed by chemo-mechanical debridement of the root canal system using non-instrumentation techniques. The canal underwent thorough irrigation with sodium hypochlorite and EDTA solutions, after which it was temporarily obturated with a calcium hydroxide-based medicament for a two-week period to promote disinfection and periapical healing. (Image 5,6)
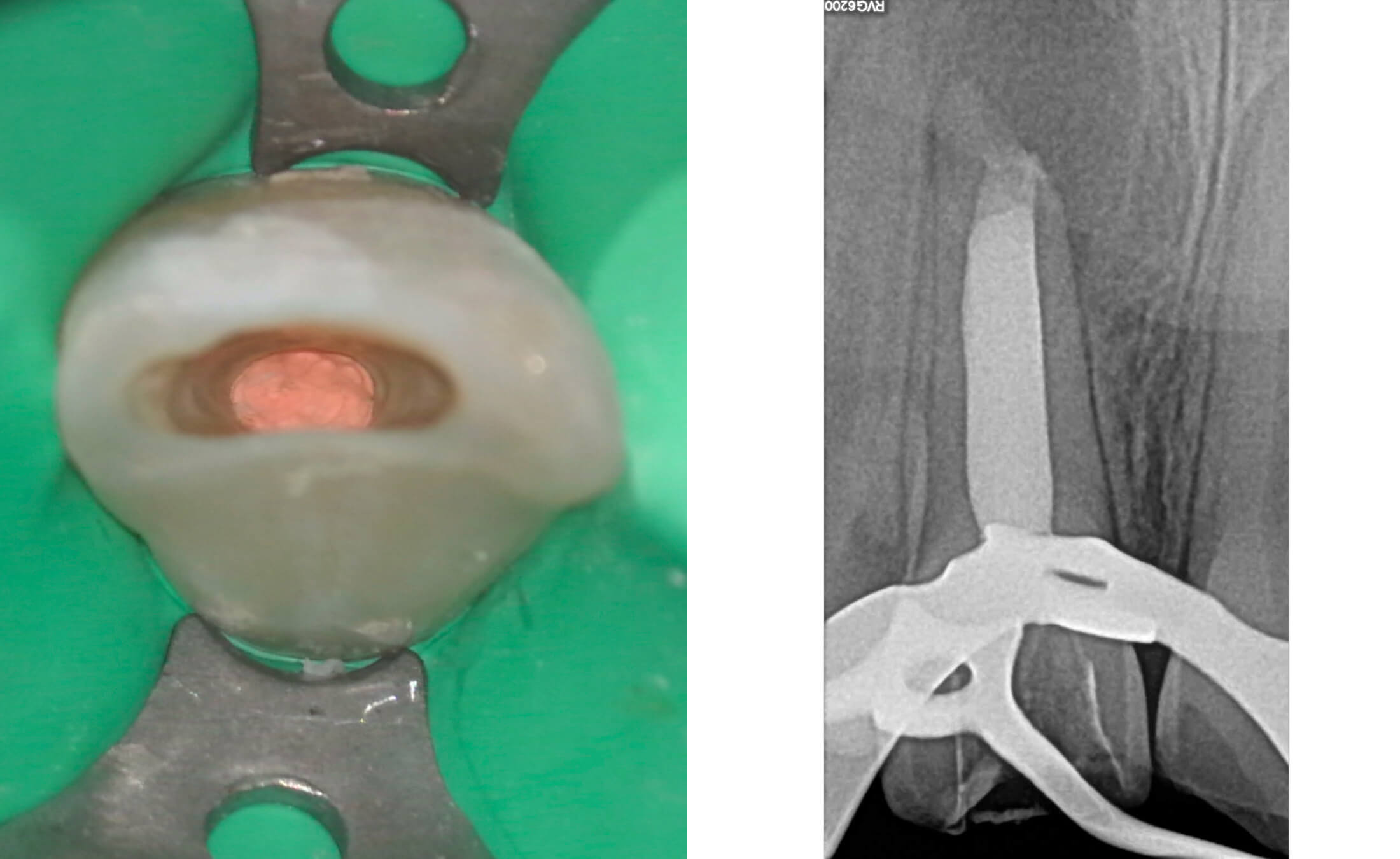
4. During the second appointment, the root canal treatment was completed. First, a 4-5 mm apical barrier was created using MTA (Mineral Trioxide Aggregate).
Following MTA setting, the remaining canal space was obturated with gutta-percha points using the cold lateral compaction technique, accompanied by an epoxy resin-based sealer (AH Plus). This approach ensures three-dimensional sealing of the root canal system. A control radiograph confirmed proper filling length with no material extrusion beyond the apex. (Image 7-10)
5. A control examination after 7 months confirmed successful bone regeneration in the periapical area of the treated tooth. Radiographic assessment demonstrated complete healing of the previous apical lesion with restored trabecular bone pattern.
Tooth #12 maintained normal pulp vitality, responding positively to cold and EPT sensibility tests. (Image 11,12,13)